Online engagement report for the review of the 2016 Statement on Consumer and Community Involvement in Health and Medical Research.
Publication Data
Executive Summary
The Statement on Consumer and Community Involvement in Health and Medical Research (the Statement)1 was developed by the National Health and Medical Research Council (NHMRC) and the Consumers Health Forum of Australia (CHF). The Statement was first published in 2006 and was last updated in 2016. It aims to support consumer and community involvement at all stages and levels of research, through highlighting the benefits and discussing a series of implementation issues.
NHMRC and CHF are revising the Statement to maintain its relevance and currency. Since the 2016 update, many organisations have produced guidelines and toolkits relating to implementation of consumer and community involvement in health and medical research. With wide availability of this information, a revised Statement will not include implementation-focussed material and will instead focus on the principles and values that underpin consumer and community involvement in health and medical research and the roles and responsibilities of all involved.
A national stakeholder engagement process was undertaken between March and June 2024 to seek views from consumers, community members, researchers, and representatives from consumer organisations, research institutions and research funders on what could be included in a revised Statement. Stakeholder engagement workshops were facilitated by the Australian Health Research Alliance (AHRA) through NHMRC’s accredited and emerging Research Translation Centres and the Australian National University, between March and May 2024. An online survey was also available on NHMRC’s Consultation Hub between March and June 2024.
Engagement activities were supported by the Review of the Statement on Consumer and Community Involvement in Health and Medical Research Position Paper (Position Paper) and Environmental Scan,2 jointly developed by NHMRC, CHF and the Consumer Statement Advisory Committee (CSAC).
The Position Paper2 posed a series of discussion questions to support engagement activities and laid out a proposed structure for a revised Statement, consisting of:
- a values statement
- a list of principles for consumer and community involvement
- a list of roles and responsibilities for consumers and community members, researchers, research institutions and funders
- a glossary.
The aim of the workshops and online survey was to gather views from a diverse range of stakeholders. Feedback from both demonstrated there is broad support for the revision, as many stakeholders feel that the Statement does not reflect current practice. Input was sought on what aspects of the current Statement did and did not work well. This feedback will enable these issues to be addressed in the revised Statement, ensuring its uptake and use by all involved in health and medical research. Suggested improvements included clearer definitions, stronger language, and inclusion of diverse perspectives, ensuring all population groups have a voice. Stakeholders emphasised how consumer and community involvement in research enhances its relevance, efficiency, and validity.
Values
Many respondents supported retaining the values of shared understanding, respect, and commitment from the current Statement, but requested more definition and context. Some suggested expanding the values to make them more explicit and adding new values. Key recommendations include defining the values, providing examples, linking them to Statement principles, ensuring relevance to all research participants, and creating mechanisms to uphold the values. New values suggested for inclusion were respect, equity, diversity, inclusiveness, accountability, transparency, collaboration, and partnership.
Principles
Respondents were largely supportive of including the example principles outlined in the Position Paper2, with some suggesting rewording to better fit the context. There was strong support for linking the principles to the values, and for detailing what each principle looks like in practice. Other suggested principles were framed around governance, capacity building and a commitment to consumer and community involvement.
Roles and Responsibilities
There was support from many stakeholders for the example roles and responsibilities suggested in the Position Paper2 for consumers and community members, researchers, research institutions, and funders to be included in a revised Statement. Some responses also suggested a revised Statement could include rights and needs for consumers and community members, researchers and research institutions. It was widely accepted that consumers and community members should be involved in all levels and stages of research but that this will depend on factors such as the type of research being undertaken. Stakeholders supported the involvement of consumers and community members at all stages of the research cycle, from planning to dissemination, and advocated for capacity-building initiatives to support effective participation where appropriate.
Ethical Considerations and Mandates
There was a strong consensus on the ethical imperative of involving consumers and community members in research, with many stakeholders advocating for research funders to mandate this involvement. Stakeholders also noted that if consumer and community involvement in research is mandated, flexibility and appropriate resourcing are essential to avoid tokenistic practices and ensure genuine engagement.
Implementation and Future Steps
Stakeholders acknowledged a need for supplementary guidance and resources to support the implementation of the revised Statement. This could include creating accessible versions of the Statement, providing training for researchers and consumers, and establishing mechanisms for monitoring and evaluating the impact of consumer and community involvement. However, due to the variance of consumer and community involvement in different types of research, specific implementation guidance will not be included. NHMRC is committed to meaningful involvement of consumer and community representatives in health and medical research, however developing contextual implementation and training resources is outside the scope of this work. This will instead be considered once the revised Statement is published.
Feedback gathered through the national stakeholder engagement process will inform the revision to the Statement, ensuring it reflects contemporary practices and meets the evolving needs of the health and medical research community. The revised Statement will promote meaningful consumer and community involvement, ultimately enhancing the impact and quality of research.
Introduction
The purpose of this report is to provide a summary of the online responses received as part of the national stakeholder engagement activities. This report has been developed by NHMRC in consultation with CHF and the NHMRC-MRFF Interim Consumer Advisory Network and is intended to complement the report published by AHRA.3
Methodology
Responses to Questions 1-16 were collected through NHMRC’s Consultation Hub and written email submissions. Analysis of the responses is presented under the 'What we heard' section. Some of the written email submissions did not follow the structure of the Consultation Hub survey, but sections of the submissions have been analysed under the questions they best fit. The survey also included demographic questions, the results of which are reported in aggregate at Appendix A.
Mixed-methods thematic analysis
All responses were manually analysed for thematic issues (with the exception of Question 4, which includes some automated analysis of commonly occurring words). The 'What we heard' section presents the qualitative analysis of responses to each question. The thematic issues have also been quantified where possible.
While not requested, many responses mentioned rights for consumers, support that researchers and institutions need to fulfil their roles and responsibilities, and the roles, responsibilities and needs of consumer organisations. The frequency of these concepts being mentioned warrants their inclusion in this report (refer to questions 8, 9 and 10).
What we heard
Question 1 – What parts of the current Statement have or have not worked well?
The feedback varied among respondents as to what has and has not worked well with the current Statement. Some respondents agreed that definitions in the current Statement are mostly clear and useful, while others suggested including more definitions to reduce ambiguity, such as definitions of ‘appropriate’ engagement and terms such as participation, involvement and engagement. Almost half of the respondents identified language as a significant downfall of the current Statement, and noted that clear, strong language is needed in the revised Statement for it to be effective. It was acknowledged by stakeholders that the current Statement was appropriate at the time it was published and useful to establish good practices but is now outdated.
Several responses said the current Statement has increased awareness of community engagement and acknowledged the important role of consumers, while others commented that they were not aware of the Statement. Those that were aware thought that the Statement’s lack of prominence and optional use have limited its impact.
Some stakeholders raised concerns about terminology, noting that the term ‘consumer’ does not include all stakeholders with lived experience. Specifically, it was suggested that the revised Statement broaden the scope of the term ‘consumer ‘and be inclusive of community members and organisations. Many suggestions were given for the replacement of the term including people with lived experience, the public, partners, patients, carers, health service users, consumers of health services or health technology, and citizens.
It was raised in several responses that the current Statement appears to focus on researchers, and that the revised Statement should address researchers, consumers and research institutions equally. Also mentioned by stakeholders was the absence of certain voices in the current Statement, and the need to show diversity, inclusivity, and respectfully acknowledge Australia’s First People and their communities.
Other suggestions for strengthening the Statement and involvement of consumers and community members in health and medical research included the need to:
- Reflect current practices and expectations, including governance and remuneration.
- Include guidance on implementation and best practice.
- Include a common language guide.
- Be accessible to all consumers and the broader community.
- Be applicable in a global context.
- Include an implementation plan and measures to ensure the new Statement is adopted consistently.
Representative stakeholder quotes4
'The current statement lacks clear definitions for the descriptions and processes involved at various levels and activities across the spectrum.'
'Language in the Statement is generally passive and places little expectation on researchers, research institutions or research funders.'
'The language is tentative and should be more definitive in expressing strategic intent, benefit, and value through involvement of the lived experience.'
'Being direct, simplifying language and avoiding interchangeable terms like "patient" and "consumer" will provide necessary clarity.'
'The term ‘consumer’ currently refers to people with distinct perspectives and lived & living experiences such as carers and community members. It is essential that the expertise of consumers, carers and community members are separately recognised & acknowledged in the Statement.'
'Different sectors use different terminology so clarity around definitions is important. For instance, in health services ‘patients and families’ are most frequently used. In maternity services, the term ‘woman’ is used. In residential aged care settings, the term 'residents’ is used. While ‘consumers’ may be the best term across health and medical research, a statement of recognition is needed regarding: the various terminology used to refer to ‘consumers’ throughout research; the positionality of the current framework in terminology choice and recommendation, as well as; the variable community preferences (within and between communities) on selected terms and the need to be responsive to community preference.'
'...remembering that if we want to involve people, we need to make sure our language does not unconsciously exclude them.'
'It needs to be co-written with consumers to ensure that it is relevant for consumers and researchers.'
'The revised Consumer Statement should expressly identify and make central Aboriginal and Torres Strait Islander consumers, community members and stakeholders as Australia’s First People. The revised Consumer Statement should emphasize our right to self-determination as it applies to community leadership and involvement in all health and medical research about us and from us.'
Resources
Stakeholders referenced several existing publications that could be referred to when drafting the revised Statement including frameworks and standards for involvement, language guides and engaging with Aboriginal and Torres Strait Islander people (listed at Appendix B).
Question 2 – Why is consumer and community involvement in research valuable?
The value of consumer and community involvement in research was clearly articulated through the responses. Stakeholders noted that the consumer and community perspective, particularly when related to lived experience of a condition, increases the effectiveness, efficiency, and validity of research. As noted by one respondent, 'lived experience is valuable in providing relevant, accurate and purposeful research.' Several responses stated that involving consumers in research is an ethical obligation to ensure research is conducted respectfully and sensitively.
Some stakeholders noted the value of involving consumers and community members in conducting their research, in areas such as data collection and 'working with researchers to make sense of the results.' Many pointed to consumer and community involvement being highly beneficial in the earliest stages of research, aligning research questions and methodology with the priorities and needs of those who will be most affected. Others mentioned the important role of consumers and community members in research translation, and the need for researchers to seek continuous feedback to ensure acceptability of the research and its outcomes. Consumers may also leverage their community expertise to communicate the results of their research to those without a scientific background and assist researchers to do the same.
Representative stakeholder quotes
'No one can understand the intricacies of living with a health condition unless they too live with it. Those with lived experience can ensure that research is of value to the community, can add, remove, edit research projects to enhance outcomes (and acceptability to the community).'
'There is a known lag in the translation of health research to practice. By involving consumers and community, we can ensure researchers are planning research based on what is meaningful, feasible and needed by locals.'
'My personal experience as a researcher is that it is also very motivating. To work directly with consumers helps to keep you focused on why you are doing the research and gives you belief in it.'
Question 3 – Why does consumer and community involvement in research matter to you?
Many of the responses to this question were similar to question 2. Additional comments included:
- Consumers and community members benefit from accessing and understanding research that is relevant to their lived condition.
- Involvement in research provides an opportunity for consumers and community members to share their unique expertise and experiences. Several shared that being involved in research after receiving a difficult diagnosis allowed them to better their own lives and the lives of others with the same condition.
- Consumer and community expertise is a vital component of research and complements the scientific and clinical expertise of researchers.
- Consumer representatives and advocates play an important role, as some consumers with lived experience are unable to be involved in the research themselves.
- Involving consumers empowers them to suggest changes to the research, reducing the power imbalance between researchers and consumers. As noted by one researcher, 'It has meant my research is much more authentic, meaningful and impactful. Based on my positive experiences embedding consumers in my research over the last 10 years I now conduct my research completely differently to how I did in the past. For example, recently I have changed a primary outcome for a study based on community engagement.'
Principles and values
Question 4 – What overarching values are essential to include in the value statement of the revised Consumer Statement, and why?
Automated text software analysis5 was used to generate a word cloud that identified the most common words mentioned in the responses (refer Figure 1). The font size is larger for the words that were mentioned most frequently. Words such as ‘research’, ‘consumer’, ‘community’, and ‘statement’ were excluded from the word cloud as their frequency obscured other terms. 'Respect', one of the values of the existing Statement, was the most common value mentioned in the responses, both in isolation and as part of common phrases, such as 'respect for lived experience.'
The other values in the existing Statement, 'shared understanding' and 'commitment', were mentioned as values that could be included in a revised Statement, but less frequently than 'respect'. This may point to a need to define or contextualise these values as they relate to consumer and community involvement in research (this is discussed further under Question 5 responses).

Some stakeholders expressed concern that including a long list of values could dilute their effectiveness and meaning: 'Too many additional values are listed here. It reads more like a ‘shopping list’ that is trying to capture everything for everyone. We recommend identifying common themes and using broader, more encompassing terms to reduce the number of listed values.'
To address this concern, the values have been broadly categorised. Several common subthemes were identified from manual analysis of the responses received through the Consultation Hub and via email, as below:
Why these values?
Many stakeholders highlighted that including these values will facilitate genuine consumer and community involvement and uphold the validity of research being conducted. The importance of lived experience, representativeness of communities, and involvement of underserved groups were key themes.
Representative stakeholder quotes
'Respect requires individuals to recognise the skills, knowledge and experience of others that may be different to their own. It requires active listening, constructive communication, valuing/managing/negotiating/embracing diverse views and input in the context of the research, and compensating consumers for their time and expenses.'
'Lived experience is a vital component of research. Consumers can help ensure that abstracts are written in a language that all will understand.'
'A value of equity ensures fair and inclusive participation, addresses systemic barriers, and promotes justice in the distribution of research benefits and outcomes, ultimately leading to research that is representative, responsive, and equitable for all communities involved.'
'Reinforcing a commitment to diverse voices in research leads to comprehensive and nuanced insights, improving the relevance and impact of research efforts. Consumers from a diverse range of backgrounds, especially those most impacted by the relevant research question, should be included in all research projects from inception, and utilised in all aspects of policy formulation and development.'
'Many consumers experience health conditions and impacts that make involvement more challenging e.g., people with communication and cognitive impairments, people who are culturally and linguistically diverse, people from non-metropolitan areas, people who live with social and economic disadvantages, people who experience digital access challenges. There is a need to recognise and support inclusion (by addressing barriers to access) of these groups to ensure that the unmet needs they currently experience are not further exacerbated.'
'Accountability ensures that the principles and values outlined in the statement are upheld and translated into concrete actions and outcomes.'
'Transparency in research processes, funding decisions, and outcomes is essential to build trust and engage consumers meaningfully. When stakeholders understand how decisions are made and how their contributions are used, it fosters stronger relationships and encourages ongoing involvement.'
'Collaboration and Partnership encourage co-creation of knowledge between researchers, institutions, and consumers, drives positive change and improves health outcomes through shared efforts and mutual respect.'
'Emphasizing a commitment to ongoing continuity engagement is vital for building and sustaining long-lasting relationships between researchers and consumers/communities. Engagement should extend beyond project-based interactions, starting from the initial stages and persisting throughout the entire research process and beyond.'
Question 5 – The values that underpin the 2016 Statement are ‘shared understanding, respect and commitment.’ How might this be strengthened and improved in the revised Consumer Statement?
Some respondents reiterated the values they would like to see in a revised Statement in response to this question. Again, the most common values listed were respect, equity, diversity, inclusiveness, accountability, transparency, collaboration and partnership.
Several responses were supportive of retaining the existing values of shared understanding, respect and commitment from the 2016 Statement, but noted without definition or context, it is unclear how they should be applied.
Stakeholder quote
'The current value statement "Shared understanding, respect and commitment" is a bit brief. It'd be good to expand on what is meant by this statement. Shared understanding of what? Respect/ commitment to whom? I realise a value statement should be concise, but it also needs to include some perspective of what is trying to be achieved.'
Some stakeholders said the existing values could be strengthened by adding more values to a revised Statement. Several common responses were identified on how the existing values (and any additional values) could be strengthened:
- The values should be defined.
- A revised Statement should include examples of the values in action.
- Any values included should be clearly linked to the Statement principles.
- The values must be relevant to all research participants.
- There should be a mechanism to uphold the values, such as ensuring they are specific or measurable so that researchers can confirm compliance.
- A small number of responses called for the values to be strengthened by making consumer involvement a requirement of research and introducing funding consequences for not involving consumers.
The most common suggestion to strengthen the values in a revised Statement (mentioned in 23 responses) was for them to be defined, followed by examples of the values in action (mentioned in 8 responses). The sub-themes identified in the previous question could be used to provide definitions and examples (refer Table 1), as could suggested definitions from stakeholder responses themselves.
Some responses link to existing documentation with values that could be adopted or adapted for a revised Statement (listed at Appendix B).
Stakeholder quote
'Clarify the existing values with expanded definitions. For example:
Shared Understanding: Define as a shared goal or vision to ensure consistent application and interpretation.
Respect: Emphasise respect for the lived experiences, perspectives, and expertise of consumers and community members.
Commitment: Specify as a commitment to meaningful collaboration and inclusion.'
Question 6 – Should values such as accountability, transparency, collaboration and partnership, equity, diversity and inclusiveness be included in the revised Consumer Statement?
Of the 89 responses received to this question, most supported these values being included in a revised Statement (either all values, or some combination of them). As can be seen in Figure 2, the value with the most support was diversity.
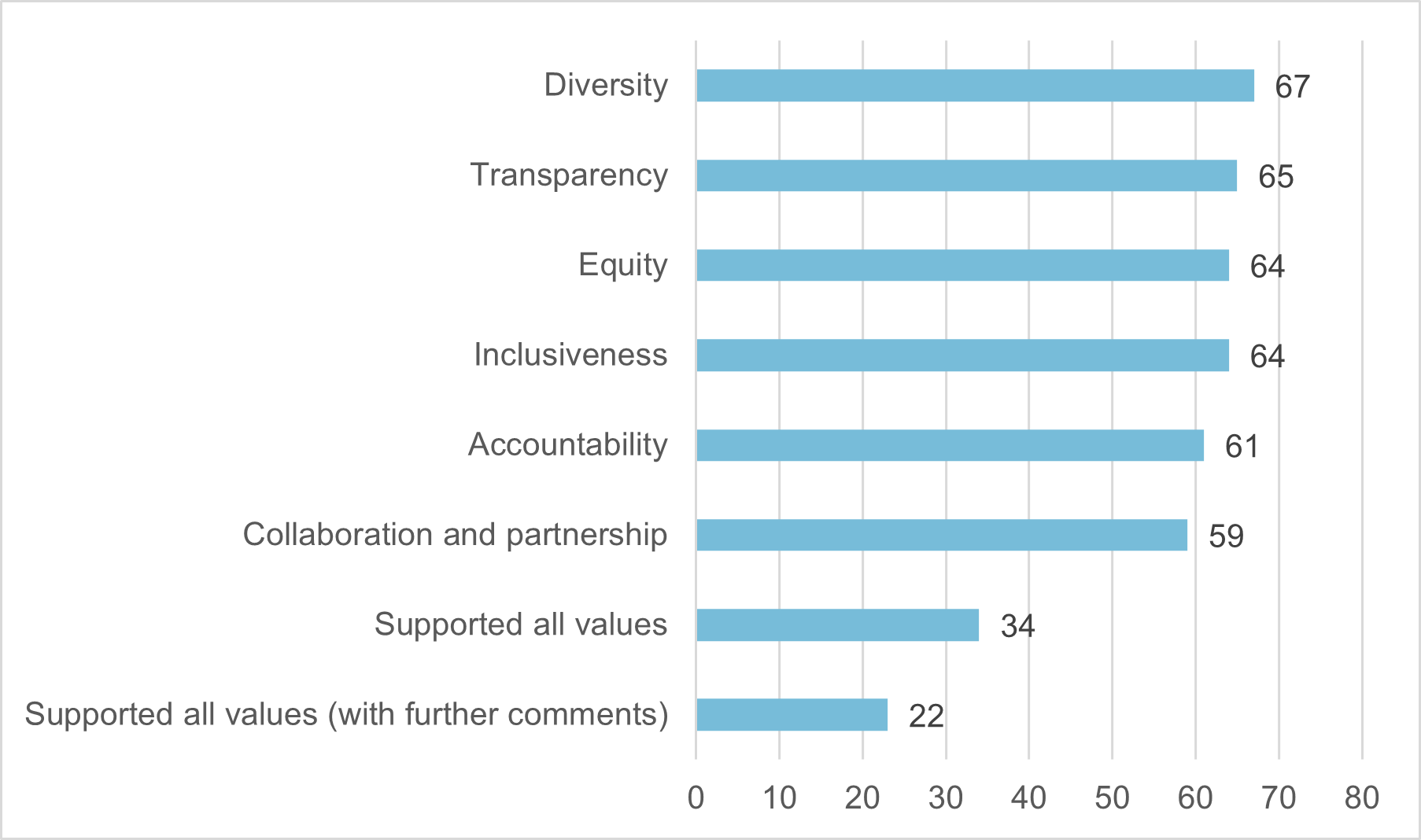
More than half of the responses (57 of 89) supported including all the values. Twenty-two of these provided further comment on how the values could be strengthened or improved, which were similar to those listed in question 4; a mechanism to uphold or measure adherence to the values, and definitions and examples of the values.
Some stakeholders listed additional values they would like included. The most common additional values were respect and respect for lived experience; with safety for consumers, accessibility, equality and trust also mentioned several times. These values align with several of the broad values and subthemes identified in responses to question 4 (refer Table 1).
Some responses to questions 4, 5 and 6 suggested that a revised Statement could be strengthened by including clear principles rather than values. A common concern was that merely providing a list of values makes them difficult to action. However, stakeholders were generally supportive of including values as long as they were clearly linked to the principles. One respondent noted: 'We suggest moving away from a focus on the values in favour of the principles. These are typically more action-oriented, objective and can be assessed which will make it clearer for people what is expected of them. These can still be linked to or paired with values, and should provide some examples that reduce the risk of abstract confusion.'
Question 7 – What do you regard as the most important principles that should be included in the revised Consumer Statement?
There was significant overlap in the responses to this question and those received to the questions about values (questions 4, 5 and 6). Some of the most common themes identified in the responses to this question were transparency, diversity, equity, accessibility, accountability, tailored consumer involvement for each research project, inclusiveness, partnership, involvement in all stages of research, and capacity building. Like the responses to questions 4, 5 and 6, stakeholders expressed they would like the values to be linked to the principles, to be defined, and for there to be a mechanism to ensure they are followed. The similarity in stakeholder feedback on values and principles will ensure they can be clearly linked in a revised Statement.
Stakeholder quotes
'We believe the principles should clearly link to the revised set of values, and should include sufficient detail to help researchers and consumers know what each principle "looks like" in practice. For example, if one of the values is "transparency" and an associated principle is something like "open and shared communication", additional details could include "sharing details about the whole research process, communicating at all stages along the research journey, having clear roles and agreed mutual expectations (such as a code of conduct), being clear about how decisions are made and who is involved.'
'Each of the principles require definitions and examples. For example, “involved” and “partnership” both have a range from minimal involvement/partnership through to co-production. The Statement should articulate these ranges and provide a minimum standard for consumer involvement/partnerships.'
'The principles should be statements that describe the overarching ideals (values) in more detail, providing further information and context.'
Position Paper – example principles
Seven principles from existing documents were included in the Position Paper2 as examples of what could be included in a revised Statement. Most of these principles are from documents that are also referenced in the Environmental Scan2, which examined Australian and international literature to identify best practice principles that could be included in a revised Statement. Most responses were supportive of including the example principles or adapted versions of each. Many stakeholders indicated their support for the principles by quoting them back in their responses, while others provided suggestions on how they could be reworded or improved for a consumer and community involvement context.
1. Consumers and community members should be involved at all stages of research (source: MRFF Principles6)
Of the 87 responses received to this question, 49 (56%) mentioned support for consumer and community involvement at all stages of research, with a further 2 indicating support for involvement in all levels of research. Stakeholders commonly mentioned the need for researchers to involve consumers early in their research, in reporting research outcomes, and in decision making.
Stakeholder quote
'Consumers and community members should be involved at all stages of research, from planning and design to implementation, analysis, and dissemination of findings. This ensures that their perspectives and needs are integrated into every phase of the research cycle, leading to more relevant and impactful outcomes.'
A small number of responses expressed the divergent view that consumer and community involvement should not be a requirement, suggesting that it may not be necessary in some types of research (such as laboratory-based research). Other stakeholders stated that consumer and community involvement should be 'tailored to the specific needs and contexts of the consumer and/or community partners to ensure relevance and effectiveness' and 'at the very least, it should be considered when developing a research proposal.'
A suggested rewording of this principle was 'Consumers and community members should be involved at all stages of research, as per consumer preference and in negotiation with consumers.'
2. Consumers and community members should be in partnership with researchers (source: MRFF Principles6)
Forty-five responses (52%) indicated support for this principle, with several stakeholders commenting that genuine partnership will ensure mutual benefit of the research and foster long-term relationships between consumers, community members and researchers.
Several responses link this principle to others presented in the Position Paper2, highlighting respect, diversity and equity as crucial to authentic partnership. One suggested combining 4 of the Position Paper2 principles to capture all concepts: 'Respect for consumers and community members with lived experience and community expertise is demonstrated by being in partnership with researchers, involved at all stages of research and representing broad diversity and equity.'
3. Consumers and community members should be involved with broad diversity and equity (source: MRFF Principles6)
Fifty-two responses (60%) mentioned support for this principle, or of diversity and equity generally. Frequent comments highlighted the importance of diversity and equity in ensuring representativeness of research and a need to involve consumers and communities who will be most impacted by it.
Stakeholders raised that diversity could mean different things depending on the research, including:
- Diverse populations such as culturally and linguistically diverse people, people in regional, rural and remote areas, Aboriginal and Torres Strait Islander people, and people who identify as LGBTQIA+
- Intellectual and cognitive diversity
- Diversity of disease severity
- Diversity of opinion.
Responses that mentioned equity noted it would ensure diversity by reducing barriers to research access: 'Researchers and funders should proactively consider the engagement strategies and resourcing required to reach diverse communities and to support them once engaged' Several stakeholders also raised the need for the Statement to provide examples of what equity principles could look like in practice.
4. Mutually respectful relationships (source: UK Standards for Public Involvement: Better public involvement for better health and social care research7)
Forty-seven responses (54%) indicated support either for this principle, or the concepts of respect, mutual respect, teamwork, and fostering positive relationships. One response suggested that this principle could be enacted by consumers, community members and researchers having clear roles and responsibilities in research. This points to a need to link the principles to not only the values, but the roles and responsibilities for everyone involved.
Another response recommended combining this principle with the second example presented in the Position Paper2: 'Partnerships between researchers and consumers and community members should be mutually respectful.' Several of the subthemes listed in Table 1 were also mentioned in stakeholder reflections on mutually respectful relationships, including addressing power imbalances between researchers and consumers, teamwork, and trust.
5. Respect for lived experience and community expertise (source: Principles of Community Engagement – CDC US Publication8)
Forty-five responses (52%) indicated support for this principle, with another 9 mentioning respect for skills and knowledge. Stakeholders acknowledged that lived experience of consumers and community members should contribute to the knowledge base of a given research topic and 'should be considered equal to the experience of other parties involved.'
Several responses raised that this principle should include understanding the physical or mental capabilities arising from a consumer’s lived experience, and a need for researchers to accommodate these. This links closely to the values of inclusiveness and accessibility in Table 1.
Remuneration was also suggested as a form of respect for lived experience: 'Payment can be a factor that encourages participation and shows contribution is valued. By offering payment, barriers such as consumer and community member work hours and caring responsibilities, are removed, enabling a more diverse consumer and community member workforce.'
6. Honesty in the development, undertaking and reporting of research, including presenting information truthfully and accurately in proposing, conducting and reporting research (source: Australian Code for the Responsible Conduct of Research9)
Forty-two respondents (48%) indicated support for this principle, or honesty and transparency in research generally. The limited number of comments that expanded on support for this principle are outlined below:
- Honesty in research requires that consumers and community members understand their role and the research, so they must have access to information in accessible formats.
- Transparency is crucial when presenting information throughout the research process to ensure trust between researchers and communities.
- Some respondents preferred the term 'transparency' rather than 'honesty.' This was also a common stakeholder view at the workshops, as noted in the AHRA report3.
7. Respect for research participants, the wider community and the environment (source: Australian Code for the Responsible Conduct of Research9)
Eighteen responses (21%) indicated support for this principle, but with few comments. One stakeholder mentioned that this appears to be an ambitious undertaking. Another noted that including this principle will encourage research participants to consider the broader impact of their research activities.
Other principles
Outside of the 7 example principles, the most common additional themes mentioned by stakeholders were:
Governance: Several stakeholders suggested including governance principles that create an expectation of consumer and community voices being embedded in the research process and organisational structures.
Capacity building of consumers, community members and researchers to support partnerships and facilitate impactful research.
Commitment to consumer and community involvement, continuous improvement, supporting partnerships, and diverse and equitable consumer involvement.
Resources
Stakeholders referenced several existing standards and publications that could be referred to when drafting the principles in a revised Statement (listed at Appendix B).
Roles and responsibilities
Several roles and responsibilities from existing documents were included in the Position Paper2 as examples of what could be included in a revised Statement. Stakeholders were asked for feedback on these examples or to provide any others they would like included.
Many stakeholders indicated their support for the example roles and responsibilities by quoting them back in their responses. Others provided specific roles and responsibilities they would like included in a revised Statement (refer to Table 2, Table 3, Table 4 and Table 5). Several responses additionally referred to the rights and needs of consumers, community members, researchers and research institutions. These are also listed in Table 2, Table 3 and Table 4.
Some general comments on roles and responsibilities included:
- consumers and community members should be able to negotiate their roles and responsibilities with researchers and research institutions
- consumer and community involvement, including the levels and stages in which consumers are involved, will differ depending on the type of research, and between individual research projects
- consumers and community members should be involved in all levels and stages of research where possible and appropriate.
Representative stakeholder quote
'…consumer and community member roles may look quite different in basic science, preclinical or greenfield research compared to applied research such as designing and testing an intervention. Articulating the roles consumers and community members may play across these different types of research will be of value to consumers and community members themselves by clarifying and managing expectations, but will also be of great use to researchers who may not always be clear on the most appropriate ways to include consumers and community members in these varying types of research.'
The Environmental Scan2 also describes possible roles and responsibilities for consumers and community members, researchers, research institutions and funders at specific stages of the research cycle. Many of the roles and responsibilities suggested by stakeholders in the online responses are more general and will be applicable to multiple stages of research. For this reason, they have been grouped thematically in Tables 2, 3, 4 and 5, rather than mapped against specific stages of research. This is also in keeping with the intention to not include implementation-focussed material in a revised Statement.
Question 8 – What roles and responsibilities for consumers and community members should be included in the revised Consumer Statement?
Stakeholders were asked to provide feedback on the following example roles and responsibilities for consumers and community members. Eighty-four responses were received to this question.
1. Consumers and community members can be involved at various levels of research activity and the institutions in which research is conducted. ‘Levels of research activity’ include planning and co-deciding, governance, developing research design and questions, recruitment, seeking funding, conducting the research, communicating the outcomes and evaluation (2016 NHMRC-CHF Statement1)
Fifty-nine responses (70%) were supportive of including a role related to involvement in various levels of the research cycle in a revised Statement. Some respondents indicated their support by mentioning consumer and community involvement in various levels and stages of research generally, or by directly quoting this example role in their response. Others listed specific roles and responsibilities which could be applied across various levels and stages of the research cycle (refer Table 2).
2. Consumers and community members should advise research institutions and researchers on their consumer and community perspectives and lived experiences (2016 NHMRC-CHF Statement1)
Thirty-six responses (43%) supported including a role or responsibility related to advising on lived experience or community expertise. Many highlighted that consumer and community involvement ensures the research is relevant, and provides a perspective that could otherwise be overlooked. It was also noted that consumers and community members should feel supported to share their lived experience to the extent they feel comfortable with.
Some respondents mentioned that individual consumers and community members should offer a balanced perspective when representing a community, noting: 'Consumers and community members should provide input based on their lived experiences, which can be used to inform and support decision making. If needed, they should bring a wider community perspective either through their own networks or by helping researchers’ source suitable perspectives.'
3. Consumers and community members may need skills, information and support in order to add value to the development, conduct and communication of research (2016 NHMRC-CHF Statement1)
Twenty-six responses (31%) supported the inclusion of this example, or mentioned that consumers and community members will need support to undertake their roles and responsibilities in a research project.
The responses presented capacity building as both a right and a responsibility of consumers and community members, noting that institutions and researchers should offer education and training, and consumers and community members should undertake it. Also noted was that consumers and community members should recognise when they require additional support or training and feel they are able to request this.
Stakeholder quotes
'Consumers and community members should be receptive to training to maximise their opportunity to contribute to research, including being prepared to learn from the researcher about their area of research.'
'Consumers should be provided with necessary information by the research team, as well as ongoing training and education to ensure skill building and equitable and informed contributions. They should be able to ask for and access any additional support or training required, and provide confidential feedback to improve CCI in the context of the research project and research institution.'
The rights of consumer and community members were commonly mentioned in the responses. Many of these rights relate to ensuring safety of consumers and community members participating in research (refer Table 2). Of note was the right to involvement that is trauma-informed, as detailed by one stakeholder: 'It is imperative that research organisations take a trauma informed approach to working with consumers. Consumers can be retraumatised by researchers, particularly if consumers are not actively involved in the early stages of the research process. Involving consumers throughout the research process should reflect trauma informed approaches.' This concept is explored further under question 10.
Question 9 - What roles and responsibilities for researchers should be included in the revised Consumer Statement?
Stakeholders were asked to provide feedback on the following example roles and responsibilities for researchers. Eighty-three responses were received to this question.
1. Champions: researchers elect to champion the benefits of consumer engagement. Key leaders with experience in consumer involvement advocate to improve the level of understanding among peers. (National Framework for Consumer Involvement in Cancer Control10)
Twenty-nine respondents (35%) supported a champion or advocacy role for researchers. Stakeholders noted that champions could be researchers on a particular project who are experienced in consumer and community involvement, while others said they should be appointed at an institutional level.
Stakeholder quote
Champions should be defined as those who have a broader influence in their organisation and beyond and hold special capacity to facilitate consumer and community involvement in programs of research or organisations or broader community conversations.
2. Combined professional development: researchers and consumers are encouraged to undertake professional development together to learn from each other’s knowledge and experience. (National Framework for Consumer Involvement in Cancer Control10)
Thirty-four responses (41%) supported including a role related to capacity building for researchers in a revised Statement. How this role could look varied among the responses, and could include researchers undertaking training on consumer and community involvement, ensuring the consumers they work with have access to training, or combined professional development for consumers and researchers. Stakeholders emphasised the benefits of consumers and researchers undertaking professional development together, noting that learning from each other’s knowledge and experience will 'enhance mutual understanding and collaboration.' It was also mentioned that research institutions have a responsibility to organise and provide access to capacity building opportunities.
3. Equality: consumers are considered equal members of the group or team (National Framework for Consumer Involvement in Cancer Control10)
Twenty-three responses (28%) supported including this responsibility for researchers in a revised Statement. Some linked the concept of equality to other commonly mentioned themes, noting that equality can be demonstrated through involving consumers and community members wherever possible and respecting their contributions, particularly in the earliest stages of research.
Some stakeholders felt that this responsibility could be strengthened by including equitable treatment of consumers and community members: 'This is important but feel it is missing the ‘equity’ lens. Researchers should also be accommodating of the needs of consumers and community members being involved. Consumers and community members working on a research project may be impacted by or care for someone impacted by a chronic condition. Therefore, researchers should factor this into their project plans and timelines, and consider any additional needs for consumers and community members.'
4. Researchers should consider how they will involve consumers and community members in the development, conduct and communication of their research (2016 NHMRC-CHF Statement1)
Twenty-three responses (28%) supported retaining this responsibility from the current Statement1. Some responses stated that consumer and community involvement will differ between projects, and this should be reflected in a revised Statement. Others supported strengthening the language, suggesting that roles and responsibilities 'must not be elective with weak words like considered'.
Many other respondents provided examples of how researchers could best involve consumers and community members in their research (refer Table 3). Many of these roles and responsibilities could be linked to the values and principles identified in earlier questions.
Question 10 - What roles and responsibilities for research institutions should be included in the revised Consumer Statement?
Stakeholders were asked to provide feedback on the following example roles and responsibilities for research institutions. Eighty-five responses were received to this question.
1. Research institutions should commit to the involvement of consumers and community members in various levels of research activity (source: 2016 NHMRC-CHF Statement1)
Thirty-seven responses (44%) supported including this responsibility in a revised Statement, or a responsibility related to commitment. Stakeholders noted that commitment to consumer and community involvement could be demonstrated through 'policy statements, strategic plans, or dedicated resources that emphasise the importance of this involvement in all research activities.'
Others noted that the language could be strengthened to 'research institutions must commit….' to create an expectation of consumer and community involvement in research. Also commonly mentioned was the need for institutions to show leadership by embedding consumer and community involvement in their organisational culture. In many responses, this concept was linked to building positive, sustainable partnerships through networking with organisations and peak bodies, and providing seed funding to facilitate consumer and community involvement at the earliest stages of research. Additional examples are listed in Table 3.
2. Seek feedback from researchers and consumer and community members involved in research and evaluate processes and outcomes (source: NIHR Cambridge Public and Patient Involvement Public Engagement Strategy 2021/202211)
Twenty-eight responses (33%) supported this role, or mentioned seeking feedback, monitoring and evaluation. One stakeholder suggested rewording this role to 'Commitment to measuring, monitoring, evaluating and continuously improving the effectiveness of involvement.' Others added 'reporting' to this role, linking it to the values of transparency, accountability and continuous improvement: 'Maintain transparency and accountability in consumer and community involvement practices. This includes regular reporting on how consumer input has influenced research processes and outcomes and open communication about the impact of consumer involvement.' Another raised the need to maintain consumer safety, suggesting that there should be avenues for both open and confidential feedback.
3. Education and training (source: National Framework for Consumer Involvement in Cancer Control10)
Forty-eight responses (56%) supported education and training, capacity building, or professional development being included as a responsibility for research institutions in a revised Statement. Several stakeholders provided suggestions on what types of education and training could be organised or run by research institutions, including:
- Combined professional development for researchers and consumers so that they may learn from each other and build relationships
- Appointing institutional champions to lead and promote consumer and community involvement in research
- Providing training for researchers on engaging with consumers and community members (this training could be co-designed and co-led by consumers)
- Integrating training on consumer and community involvement into undergraduate and postgraduate university courses
- Training that is specific to a research project, such as working with consumers and community members with disability or lived experience with a particular condition
- Cultural sensitivity training.
Several responses also mentioned the need for trauma-informed approaches to research. This was also presented as a right for consumers and community members and a responsibility of researchers (refer to questions 8 and 9). Stakeholders noted that providing training on trauma-informed practice, and wellbeing support for consumers and researchers, is a responsibility of research institutions.
Outside of the example roles and responsibilities, a commonly mentioned role for research institutions was providing the necessary infrastructure to support consumer and community involvement. Of note was the need for institutions to streamline their policies and processes to ease the administrative burden on consumers, community members and researchers. However, some respondents noted that institutions may need additional funding and resources to be able to perform their roles and responsibilities more effectively.
Question 11 – What roles and responsibilities for research funders should be included in the revised Consumer Statement?
Stakeholders were asked to provide feedback on the following example roles and responsibilities for research funders. Ninety responses were received to this question.
1. Policy and Processes: Through policy guidance and other processes, set expectations for how people with lived experience (PWLE) and consumers should be involved in research projects. (Adapted from: Lived Experience Involvement in Research Funding: Taking a more systematic approach12)
Forty-six responses (51%) supported this role for research funders, or mentioned policy, guidance and setting expectations. Stakeholders also listed areas they would like more guidance material in (refer to Table 5, advocacy and leadership).
Stakeholders also noted that consumers and community members may not always be involved to the same degree in basic science research as they are in clinical research, and expectations set by research funders should reflect differences in research types. Further, in some disease-specific research it may be difficult to recruit people with lived experience, with one stakeholder noting they have experienced 'challenges in recruiting consumers with lived patient experiences of low-survival cancers, consumers with experience of conditions that are extremely rare in Australia, or conditions that place a high burden on carers.' While most stakeholders agreed that people with lived experience should be involved in research wherever possible, several noted that funders may need to acknowledge these challenges when setting expectations.
Thirteen respondents stated that funders have a responsibility to mandate consumer and community involvement in the research they fund. It was noted that additional funding and resourcing may be required if funders are to make consumer and community involvement a condition of funding (refer to Table 5, support research). The prospect of mandating consumer and community involvement is explored in detail under question 14.
2. Research Funding Programs: Research funders can involve consumers in reviewing funding applications, setting priorities, identifying research topics, designing and developing programs, and supporting funded projects (Adapted from: Lived Experience Involvement in Research Funding: Taking a more systematic approach12)
Thirty-six responses (40%) supported research funders involving consumers and community members in their own processes. As noted by one stakeholder, 'while stating principles and values that researchers should adhere to is useful, the NHMRC has a responsibility to publicly state their own commitment to consumer and community involvement.' Several responses suggested strengthening the wording to 'research funders must involve consumers.'
Of the processes that consumers and community members could be involved in, peer review was the most frequently mentioned. Stakeholders supported consumer involvement being given significant weight in grant assessment, and consumers and community members being involved as scoring members with separate assessment criteria. It was also noted that funders could support peer review by providing training and guidance to grant application assessors (both scientific and consumer) on evaluating consumer and community involvement.
Tables
Shared roles and responsibilities
The example roles and responsibilities were broken down by each contributor to research: consumers and community members, researchers, research institutions, and research funders, except for the below shared responsibilities:
1. 'Research institutions, researchers, consumers and community members all have a responsibility to consider the best person(s) for a particular role or task, taking into consideration issues such as age, gender, disability, cultural background and experience, health system experience and availability' (source: 2016 NHMRC-CHF Statement1)
Twenty-two responses (26%) supported this being included as a role for consumers and community members in a revised Statement. Despite this support, several responses noted that consumers are not always in a position to consider the best person for a role, with one stakeholder noting: 'This doesn’t read right from a consumer perspective, as consumers don’t have the power to do this.'
Other stakeholders reframed this, saying that consumers and community members have a responsibility to consider whether they are the best person for a role on an individual level, with one response noting: 'Consumers and community members need to recognise the diversity within their community and ensure the most appropriate representation is achieved for any specific research initiative. This may mean that their own personal involvement is not included.' One response called for clarification on what the 'best' person for a role means, and others noted this will vary depending on the research; it could be the most experienced person, a community representative, or someone with lived experience of a condition. One response suggested drawing on the NHS Health Research Authority Principles for Public Involvement13, which focus on involving the right people, and the right amount of people, to maximise effectiveness of the research.
Twenty responses (24%) supported this being included as a role for researchers in a revised Statement. Some linked it to the values of diversity and lived experience, through ensuring the relevant community is represented in the involvement of consumers. Others noted that researchers could find the best person for a role by building partnerships with consumer organisations and networks.
Fifteen responses (17%) supported this being included as a role for research institutions in a revised Statement. Some noted that institutions have a responsibility to facilitate the partnerships that enable researchers to recruit suitable consumers and community members for their research: 'Research institutions must act as administrators to facilitate engagement by establishing avenues or mechanisms for ongoing dialogue and collaboration between researchers and consumers/ community members. This will prevent duplication and avoid overburdening consumers them with excessive demands or responsibilities.' Other respondents noted that institutions have a responsibility to provide training for consumers and community members so that they may best perform their role in research.
2. Governance: governance structures, including boards and committees, policies and procedures, incorporate the principles, values and elements for effective consumer participation (source: National Framework for Consumer Involvement in Cancer Control10)
Thirty-three responses (32%) supported this being included as a role for research institutions, and 19 responses (21%) supported this being a role for research funders. One stakeholder suggested strengthening the language to 'consumers must be members of all levels of governance structures…' It was also mentioned that institutions and funders can demonstrate a commitment to the consumer and community involvement they expect of researchers by involving consumers in governance.
Several responses linked governance structures to co-design and shared decision-making with consumers and community, as noted by one stakeholder: 'These [governance structures] should be established in consultation with various consumer cohorts to ensure they truly reflect the needs and preferences of the communities involved.' Another noted that research institutions should provide governance training to researchers to ensure they understand and adhere to requirements, including policy, processes and ethics requirements. Additional suggested roles for research funders in governance included providing guidance on different types of consumer and community involvement, and remuneration guidelines.
Roles, responsibilities and needs of consumer organisations
The role of consumer organisations in research was mentioned frequently in stakeholder responses. It is noted that Health Consumers NSW (HCNSW) and the NSW Users and AIDS Association (NUAA) convened their own workshop of 15 consumer organisations to prepare a submission to the review of the Statement.
Respondents highlighted that consumer organisations are increasingly being involved as research partners and can be involved in the same ways as individual consumers and community members, and throughout all stages of the research cycle. Consumer organisations are uniquely placed to connect researchers with consumers and community members, and to advise on best practice consumer and community involvement.
Stakeholder quotes
'As a consumer organisation, we can provide the perspective of a larger consumer cohort and represent their interests. We are also able to connect researchers with a diverse range of consumers in our community.'
'Consumer organisations that work with consumers and represent the interests of consumers in the research process are critical partners and should be recognised in the Statement.'
Stakeholders from consumer organisations mentioned their positive experiences in research, highlighting 'the importance of amplifying the perspectives of people with lived and living experience to ensure meaningful and relevant research.' However, they also noted that consumer organisations require more funding and resources to do so effectively. Responses drew attention to some specific challenges faced by consumer organisations:
- Receiving requests from researchers for consumer and community involvement without adequate funding or resources.
- An expectation that consumer organisations will provide in-kind or financial support to NHMRC-funded grants. This can be a barrier to involvement of organisations that lack sufficient funding or resources.
- Consumer organisations need to support consumers and community members with training and mentoring so they may be involved in research, and they require more time, funding and resources to do so. Several responses called for this funding to be provided by NHMRC.
Resources
Stakeholders referenced several existing publications that could be referred to when drafting the roles and responsibilities in a revised Statement (listed at Appendix B).
Ethical considerations and expectations
Question 12 – Should involvement of consumers and community representatives be an expectation of research?
This question included tick boxes where respondents could select 'yes', 'no', or 'not sure'. Of the 93 responses, 86 (93%) selected 'yes,' 2 (2%) selected 'no,' and 5 (5%) selected 'not sure.' Eighty-seven respondents also provided written comments.
The majority of responses received to this question emphasised the importance of involving consumers and community members in all health and medical research. It was noted that involvement enhances the relevance, safety, and outcomes of research, ensuring it aligns with real-world experiences and needs. Consumers provide valuable insights and have connections to communities, aiding in recruitment and translation of research results. Responses also argued for leadership, not just involvement, of Aboriginal and Torres Strait Islander community organisations in research related to them. Several responses to questions 12 and 13 quoted the expression 'nothing about us, without us'.
Responses that said consumer and community involvement members should not be an expectation of research highlighted issues surrounding resourcing, coordination, bias, lack of training and support, and varied participation levels. It was also raised that participation is not always relevant to the project being undertaken, but noted that there should be justification provided if consumers and community members are not included.
Question 13 – Is there an ethical imperative to involve consumers and community representatives in research?
This question included tick boxes where respondents could select 'yes', 'no', or 'not sure'. Of the 94 responses, 84 (89.4%) selected 'yes,' 3 (3.2%) selected 'no,' and 7 (7.4%) selected 'not sure.' Eighty-one respondents also provided written comments.
Most respondents agreed that there is an ethical imperative to involve consumers and community members in research. This involvement ensures that the research is not only scientifically sound but also socially relevant and respectful of the communities it aims to benefit.
Stakeholders noted that appropriate involvement of consumers and those with lived experience in the design, management, and conduct of research ensures it addresses both perceived and actual community needs. This ethical imperative was supported by the concept of an 'ethic of responsibility,' which emphasises the duty to consider various perspectives in health and medical research. Building trusting relationships and fostering two-way learning between researchers and consumers is crucial for authentic engagement and ethical research practices.
Responses that said there is not an ethical imperative to involve consumers and community representatives in research varied. Some stakeholders thought that it should be dependent on the type of research and that ethics committees should make an assessment on whether involvement is warranted. Concerns were also raised about the ethics of funders demanding that researchers include consumers without any training or evidence of competency, and in parallel, not provide consumers with adequate knowledge of research in order to optimise their experiences and contributions.
Mandating consumer and community involvement in research
Question 14 – Should funders of research mandate the involvement of consumer and community representatives in the research they fund?
This question included tick boxes where respondents could select 'yes', 'no', or 'not sure'. Of the 92 responses, 70 (76%) selected 'yes,' 13 (14%) selected 'no,' and 9 (10%) selected 'not sure.' Eighty-six respondents also provided written comments.
The responses that supported or were unsure about a mandate were varied. These ranged from strongly supporting a mandate in all research types, to supporting this where possible but noting that exceptions or allowances may need to be made. Many stakeholders also mentioned additional funding and resourcing may be needed if consumer and community involvement is mandated. Several suggested softening the terminology, noting that consumer and community involvement could instead be incentivised, required, expected, or encouraged.
Responses that strongly supported a mandate
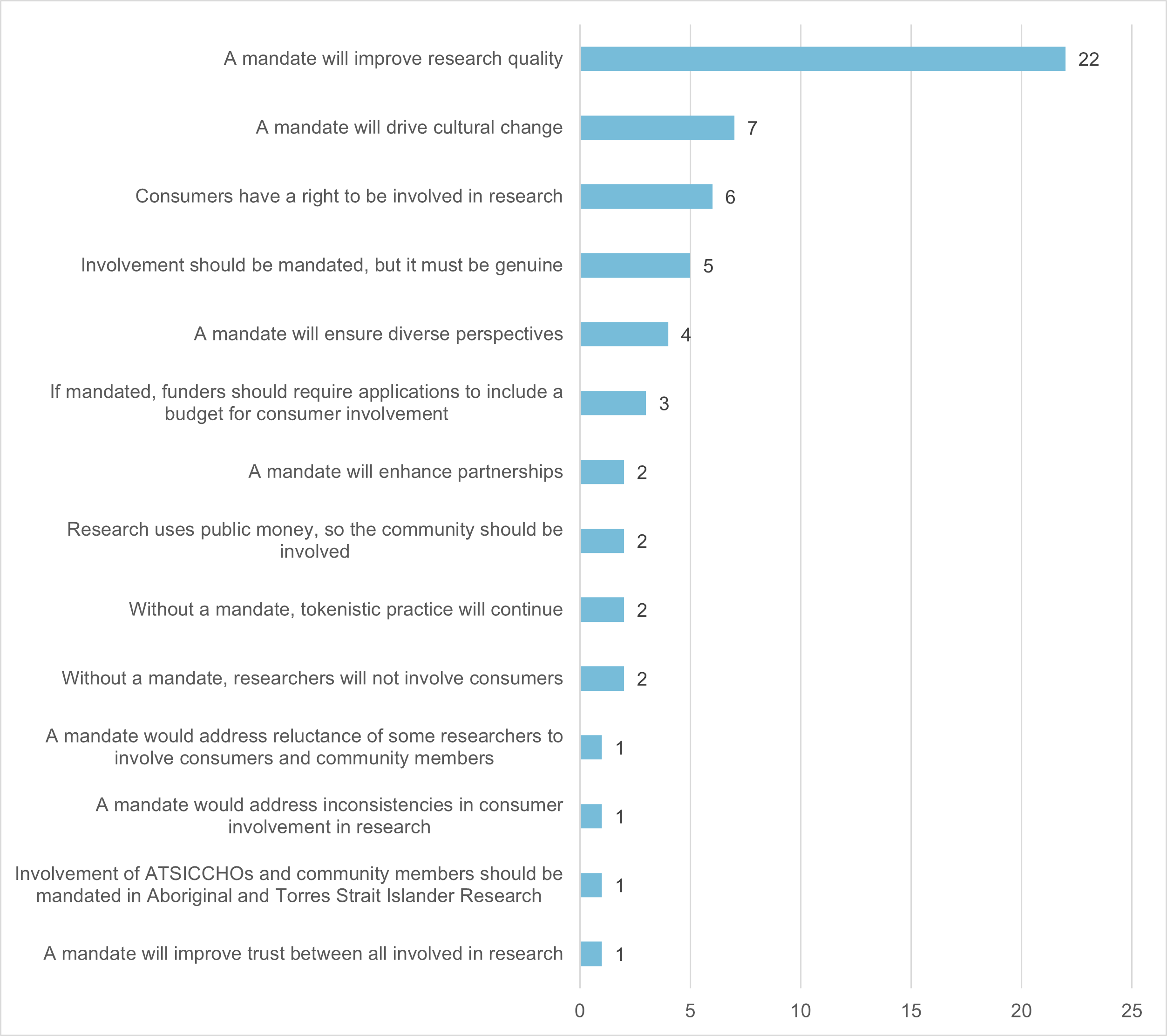
Among these responses, the most frequent comment was that consumer and community involvement will improve the quality of research. Others linked a mandate to the rights and safety of consumers and community members, particularly when the research is about a particular medical condition or involves marginalised populations. Some stakeholders expressed the opinion that a mandate is necessary because some researchers choose not to involve consumers and community members in their research. These comments from stakeholders and the frequency they were mentioned are presented in Figure 3, and some representative comments are below.
Representative stakeholder quotes
'Individuals have a right to be involved in research that affects them. Nothing about us without us.'
'Mandating the involvement of consumers, carers and community members in research funding will ensure that CCI is viewed as essential to research, rather than an optional 'add on'. Research into which consumers, carers and community members have meaningful input - as partners with researchers - will be more relevant and appropriate, leading to more effective translation into practice and better health outcomes for the most affected population.'
'If it’s not mandatory, researchers will choose not to involve consumers, or involve them in a minimalistic or tokenistic manner to secure funding for their project.'
'Mandating involvement ensures that diverse voices, especially those from underrepresented or marginalised groups, are heard and considered in the research process.'
'Mandating can feel like a very strong action but is necessary initially to help achieve the long-term goal of wholesale culture change (i.e. CCI embedded in health and medical research).'
'Funding must be tied to the provision of evidence of genuine CCI collaboration, for example via early-stage workshops, meeting minutes, media updates.'
Responses that supported a mandate with additional support and flexibility
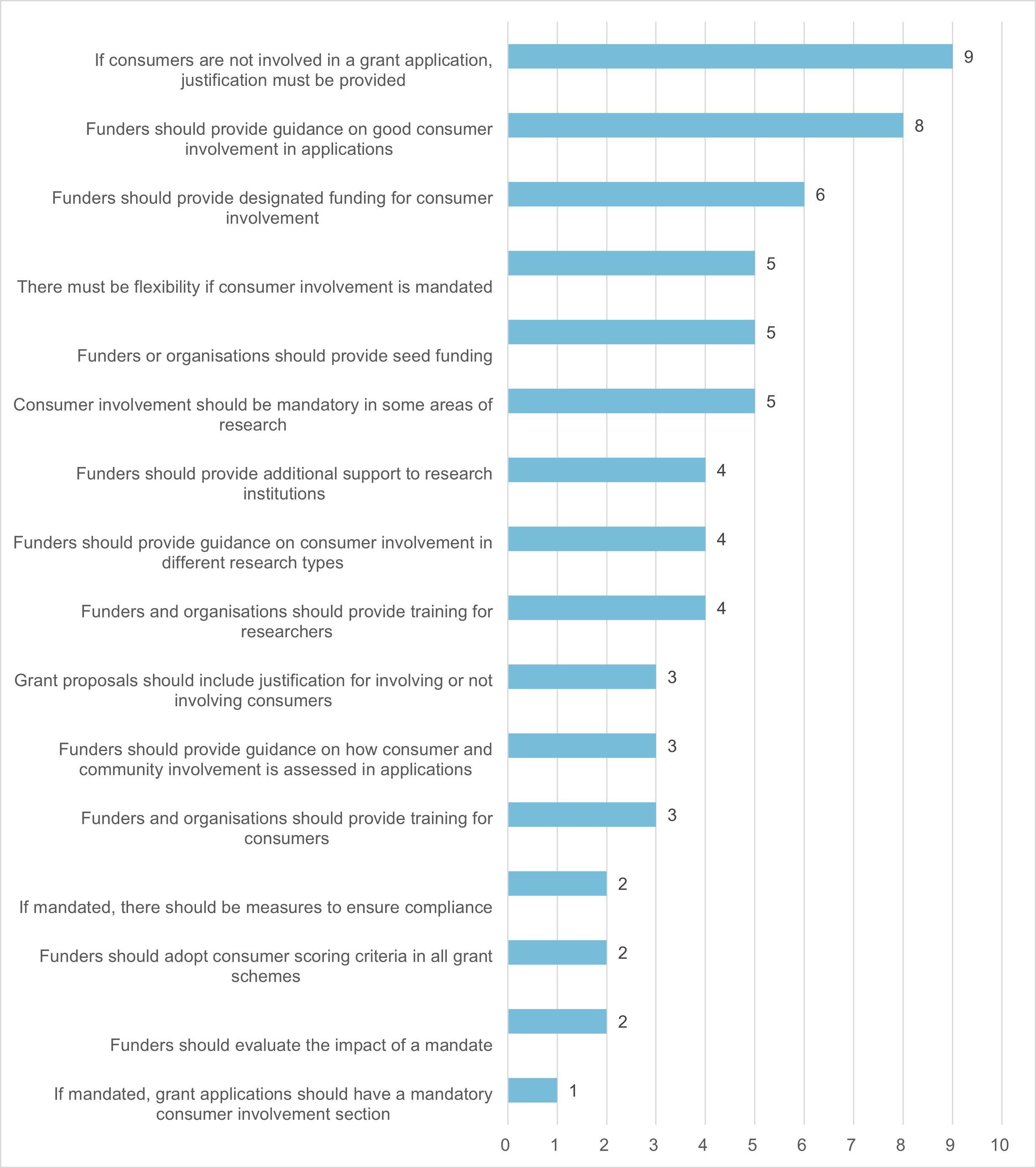
While most respondents supported consumer and community involvement being mandated, stakeholders expressed concern about this occurring in isolation. Responses highlighted that researchers would need time, resources and funding to build capacity in consumer and community involvement. Seed funding was mentioned several times as a mechanism for researchers to better involve consumers and community members in the very early stages of research. Some responses called for funders to support researchers and consumers through funding, training, and targeted research. Others said that a mandate must be supported by more guidance on involving consumers and community members.
Another common theme was that a consumer and community involvement mandate must be flexible. Some respondents said it should be mandated in certain research types, such as clinical research. It was noted that consumer and community involvement may not always be possible, and researchers could be required to provide justification for not doing so when applying for grant funding. Comments from stakeholders about resourcing and flexibility to support a mandate are presented in Figure 4, and some representative comments are below.
Representative stakeholder quotes
'It is important that consumer and community involvement is adequately resourced, supported, and meaningful. Funders need to revise funding structures and provide research institutes with adequate support around implementing these practices to avoid tokenistic involvement. Funders also need to provide clear guidance on consumer and community involvement is assessed and weighted.'
'There should be a mandate that communities should be consulted and involved in research that impacts them, also acknowledging that the type and extent of involvement may be influenced by the stage or nature of the research, resources, and the desire/needs/capacities of those communities to be involved.'
'Involvement of consumer and community representatives should be a default expectation, with an obligation on the research funder to explain why it is not required in any specific scheme or research project; the ‘if not, why not? approach.'
'Broadly, we believe that CCI should be a mandated part of health and medical research, but mandates that do not allow for the inherent flexibility required in co-produced approaches to research should be avoided. Funders should support CCI in ways that are adaptable to the specific needs and context of each research project.'
'Currently, there are very few mechanisms for funding the involvement of consumer and community representatives in the early co-design/development of grant proposals, and this is a major barrier to meaningful consumer involvement in this part of research process. Should funders mandate consumer involvement in research, it is critical that seed funding is prioritised to facilitate their involvement in grant development.'
Responses that did not support a mandate
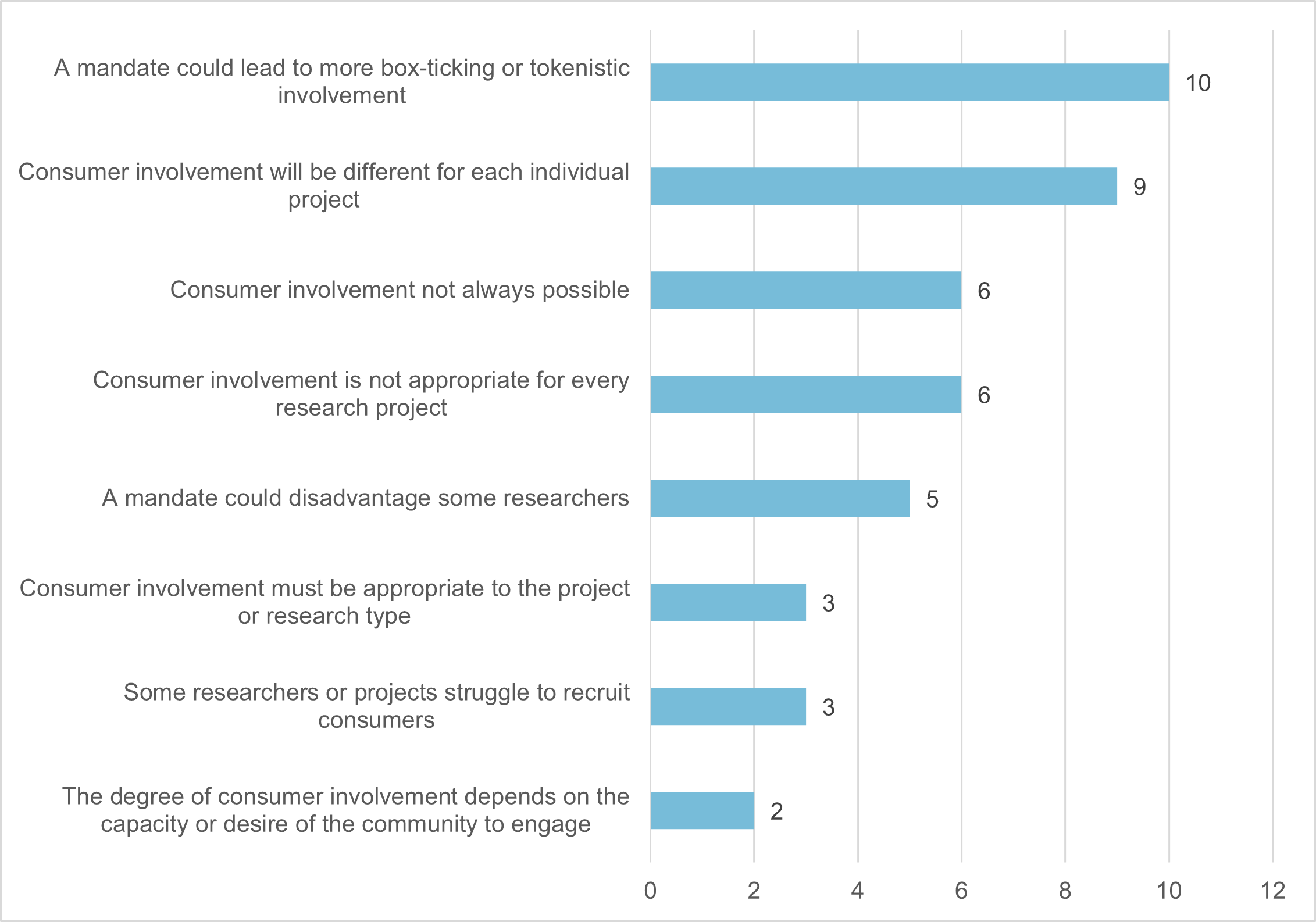
Stakeholders who did not support a mandate were primarily concerned with potential tokenism, suggesting that researchers may involve consumers and community members only to secure funding. Another common concern was that a mandate would disadvantage researchers who are unable to recruit consumers and community members, or who research in a field that does not easily lend itself to consumer and community involvement. All these responses acknowledged the value of consumer and community involvement but called for it to be appropriate to each research project. Comments from stakeholders who did not support a mandate are presented in Figure 5, and some representative comments are below.
Representative stakeholder quotes
'While consumer involvement is important, there are times and good reasons when it may not be possible. There is also a risk that if CCI is mandated, poor/tokenistic practices will continue. The right incentives need to be used to encourage, promote, support and reward good consumer involvement in health research.'
'In some biomedical research or some research involving development of methods, such "participation" would be tokenistic as it is difficult for the consumers to have a meaningful and substantial influence on the research activity.'
'I believe that this would disadvantage researchers who are unable to find consumers and community representatives who want to be involved.'
Implementing the revised Statement
Question 15 – How should researchers involve consumers and community representatives in their research?
Many of the responses to this question overlapped with questions 9 and 10: What roles and responsibilities for researchers should be included in the revised Consumer Statement? and What roles and responsibilities for research institutions should be included in the revised Consumer Statement? Again, many responses focused on consumers and community members being involved throughout the research cycle (particularly in the earliest and latest stages of research), and at different levels including governance and steering committees. Some additional suggestions from stakeholders are below.
Researchers can adopt non-conventional methods of recruiting consumers and community members, such as advertising through mainstream media or social media, at community events, and at healthcare clinics. The importance of sharing accessible information about the research with consumers and the purpose of their involvement was also highlighted. Some responses noted that researchers sometimes have difficulty recruiting consumers and community members, and suggested that research institutions address this with designated staff for consumer involvement. Part of this role could involve matching consumers and community members to appropriate research teams based on their lived experience or interests, facilitated by a database for consumers and community members to register their interest. Research institutions may also consider creating a consumer panel or group to advise on research projects.
Other responses mentioned the importance of researchers building long-term relationships with consumers and community members independent of a single research project: 'Research institutions/centres should enable, facilitate and maintain regular opportunities for discourse between researchers and consumers to foster a collaborative approach, develop relationships, and enable consumer input from research idea inception.' Stakeholders also noted open communication should occur throughout each research project, with consumers being updated and involved at all stages including data collection, analysis and interpreting results.
A key theme noted throughout the online engagement responses is that consumer and community involvement will differ based on several variables, such as the type of research and ease of recruiting consumers. Acknowledging this, and tailoring consumer and community involvement to each research project, was presented as being crucial to genuine, transparent involvement. As noted by one stakeholder: 'Researchers should aim for the highest level of involvement that they can authentically offer - honesty is important here so as to build trust and avoid tokenism, e.g. don't call it co-design if it is consulting and don't call it partnership if it is engagement.' Many respondents agreed that consumers and community members should be involved when the research impacts on them or relates to lived experience. Involving multiple consumers and community members where possible was also mentioned to reduce the power imbalance in the research team and ensure diverse perspectives.
Several responses noted the difficulties of meaningfully involving consumers and community members in basic science or laboratory-based research, due to the complex subject matter and lack of immediate relevance. Stakeholders provided some suggestions on how researchers may involve consumers and community members in their basic science research, including education, explaining the long-term intent of the research, and ensuring the research is ethical.
Representative stakeholder quotes on basic science research
'If it is 'deep' basic science research then the 'consumer' may be taken as the upstream users of the research outcomes or knowledge in the pathway to translation. Consumers can also be good sources of litmus test for community expectations, values and reactions to ethical questions that may arise in the course of pure basic scientific research.'
'Discussing the potential long-term outcomes [with consumers] that could flow from the proposed fundamental research, finding out if this will address a need.'
'Research buddy: a less formal way of obtaining the community perspective. Researchers may arrange meetings two or three times per year with the buddy/s to discuss the progress of the research and its findings. This method is particularly helpful in laboratory-based research or projects using linked data.'
Question 16 – What issues should be considered once the revised Consumer Statement has been finalised and published?
Responses to this question agreed that the revised Statement should be widely promoted and supported with additional material and resourcing to ensure its uptake by all involved in health and medical research. Common responses regarding post-revision issues have been grouped thematically below.
Evaluation and compliance
Stakeholders called for the revised Statement to be accompanied by a plan for how its use and impact will be monitored and evaluated. This could include 'seeking continuous feedback from consumers and researchers to improve practices' and 'a standardised approach to reporting on consumer engagement within grant deliverables reporting.' Several responses said that the Statement should be revised more frequently to reflect updates in language or practice. Stakeholders also noted that compliance with the revised Statement should be monitored through reporting, particularly if consumer and community involvement is made mandatory in health and medical research.
Dissemination
As noted in responses to question 1, 'What parts of the current Statement have or have not worked well?', many stakeholders were unaware of the Statement or had not used it in their research. Stakeholders called for the revised Statement to be widely disseminated through a variety of media so that all intended audiences are reached. Suggestions for NHMRC and CHF to consider included:
- Publishing accessible versions, such as easy read, shortened, and audiovisual versions
- Publishing versions in languages other than English
- Communicate the publication of the Statement widely, and ensure stakeholders are aware it is a resource for everyone involved in research
- Promote stories or case studies that demonstrate the values, principles, roles and responsibilities of the revised Statement
- Hold a conference or webinar to launch the revised Statement
- Hold discussions with research institutions and funders about how they intend to use the revised Statement in the research they support
- Commit to ongoing communication of the Statement to ensure consumers and researchers entering the sector are aware of it.
Implementation
Stakeholders noted the proposal not to include implementation-focussed material in a revised Statement. Commonly mentioned was the importance of providing guidance that demonstrates what the content of the revised Statement may look like in practice. Some responses called for this material to be included in the revised Statement itself, while others said this could be accompanying material. Suggestions from stakeholders around implementation included:
- Updating the Toolkit for Consumer and Community Involvement in Health and Medical Research14.
- National guidance on consumer remuneration.
- Developing a central repository for resources, guidance documents, and self-nominations for consumers and community members who are interested in research. One stakeholder suggested this could be a 'living library' to align with the 'rapidly evolving practice of consumer engagement and involvement internationally, and to help avoid further duplication in effort by research institutes, networks and communities of practice in creating their own resource libraries.'
- Guidance material on how to involve consumers and community members in specific types of research or research activities. This material could be produced by NHMRC and CHF, or the revised Statement could include guidance on where to find material published by other organisations.
- Funders should commit to the Statement implementation by co-designing their implementation strategies with consumers and community members, and involving them in other processes such as peer review.
Funding
Many stakeholders called for a revised Statement to be supported by more funding (particularly from NHMRC) for consumer and community involvement in research. Most of these responses mentioned that consumer organisations require funding to build infrastructure for involvement and to participate as partners in NHMRC-funded grants. Some respondents also called for more targeted funding for consumer-led research, particularly in marginalised populations.
Many responses also noted funders (particularly NHMRC) could fund capacity building to improve uptake of the revised Statement. Suggestions from stakeholders included:
- Training for researchers and consumers on implementation of the revised Statement
- Online tutorials on the grant application process
- Developing an accreditation process for consumer and community involvement in research.
Improving the research experience of consumers and community members
The most common response under this theme was specific to NHMRC’s grants management system, Sapphire. Consumers and community members noted when making a Sapphire profile they must provide information about their institution, publications and track record, which are often not applicable. Many responses called for this system to be updated, particularly if consumer involvement is to be expected or mandated in research: 'This system needs to be reviewed in partnership with consumers and consumer-led organisations to ensure that it is accessible for consumers and consumer researchers.' Respondents also provided suggestions on how the track record of consumer and community members could be considered in grant applications: 'Many consumers with lived experience become involved in research through their lived experience and may have many years of experience as a consumer representative but limited publications.' Several responses also noted research funders should involve consumers as scoring members in peer review to demonstrate they value consumer and community involvement and are committed to it.
Appendices
Appendix A - Demographic data analysis
Ninety responses were received through the Consultation Hub: 49 from individuals and 41 on behalf of an organisation. A further 12 written responses were received from organisations via email, but as they did not complete the demographic questions, they have not been included in this analysis.
Of the 90 survey respondents, 37 (43%) had attended an AHRA workshop, or someone from their organisation attended. Two respondents (2%) planned to attend an AHRA workshop but had not yet at the time of their submission.
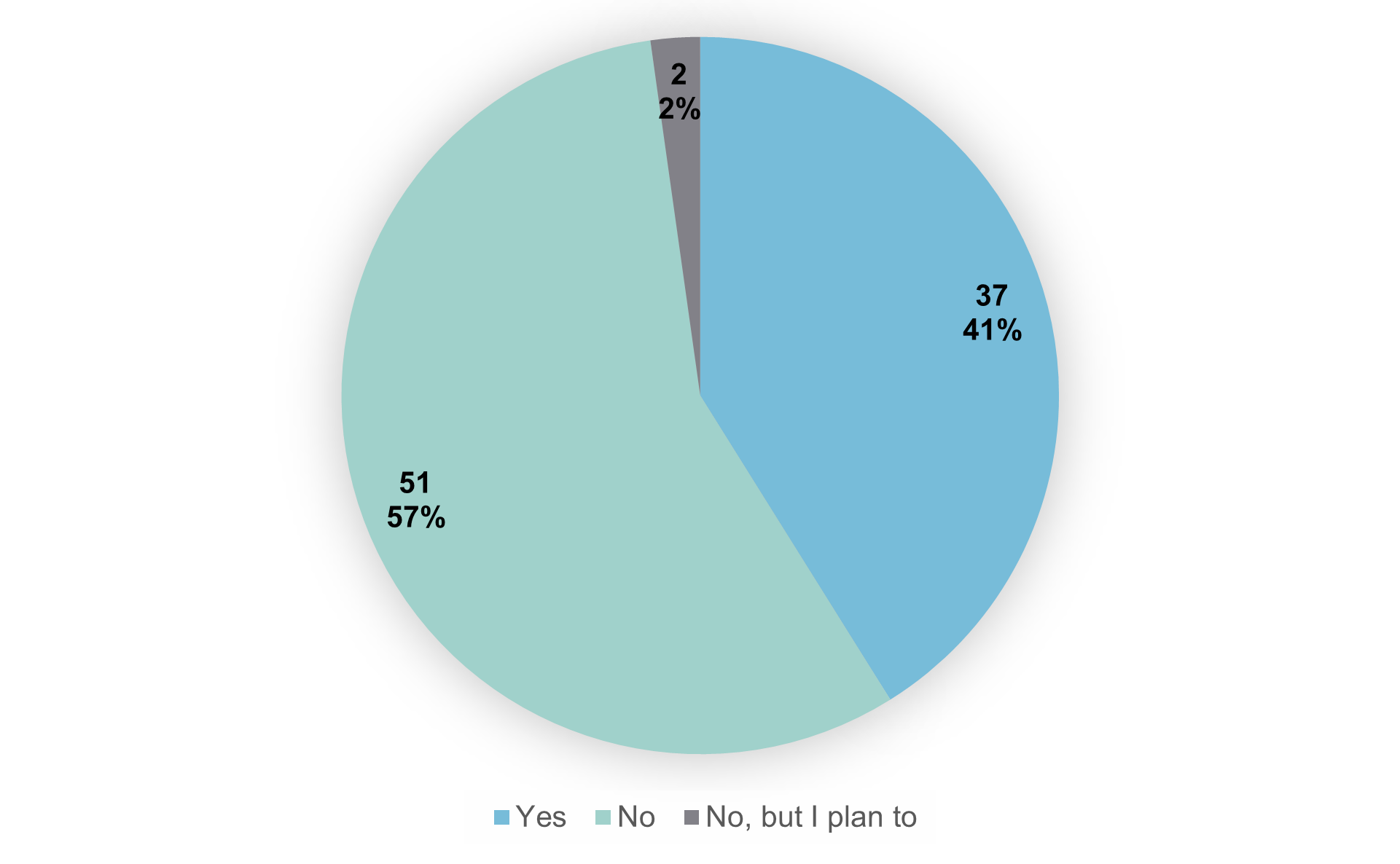
Responses from individuals
Individual respondents were invited to complete a series of optional demographic questions.
Stakeholder type
Individuals could select multiple stakeholder roles (refer Figure 7). Of the 45 responses received to this question, 25 (56%) respondents identified as a consumer, consumer representative, community member, another role, or some combination of these roles. Two respondents (4.5%) identified as both a consumer and a researcher, with one respondent (2%) identifying as a consumer, consumer representative and researcher. Ten respondents (22%) identified as a researcher only, and 5 (11%) identified as some combination of researcher, research administrator, research funder or other roles. Two respondents (4.5%) selected 'other' only. Self-identified 'other' roles included individual with lived experience, Health Research Ethics Committee (HREC) community representative, mental health professional, and carer.
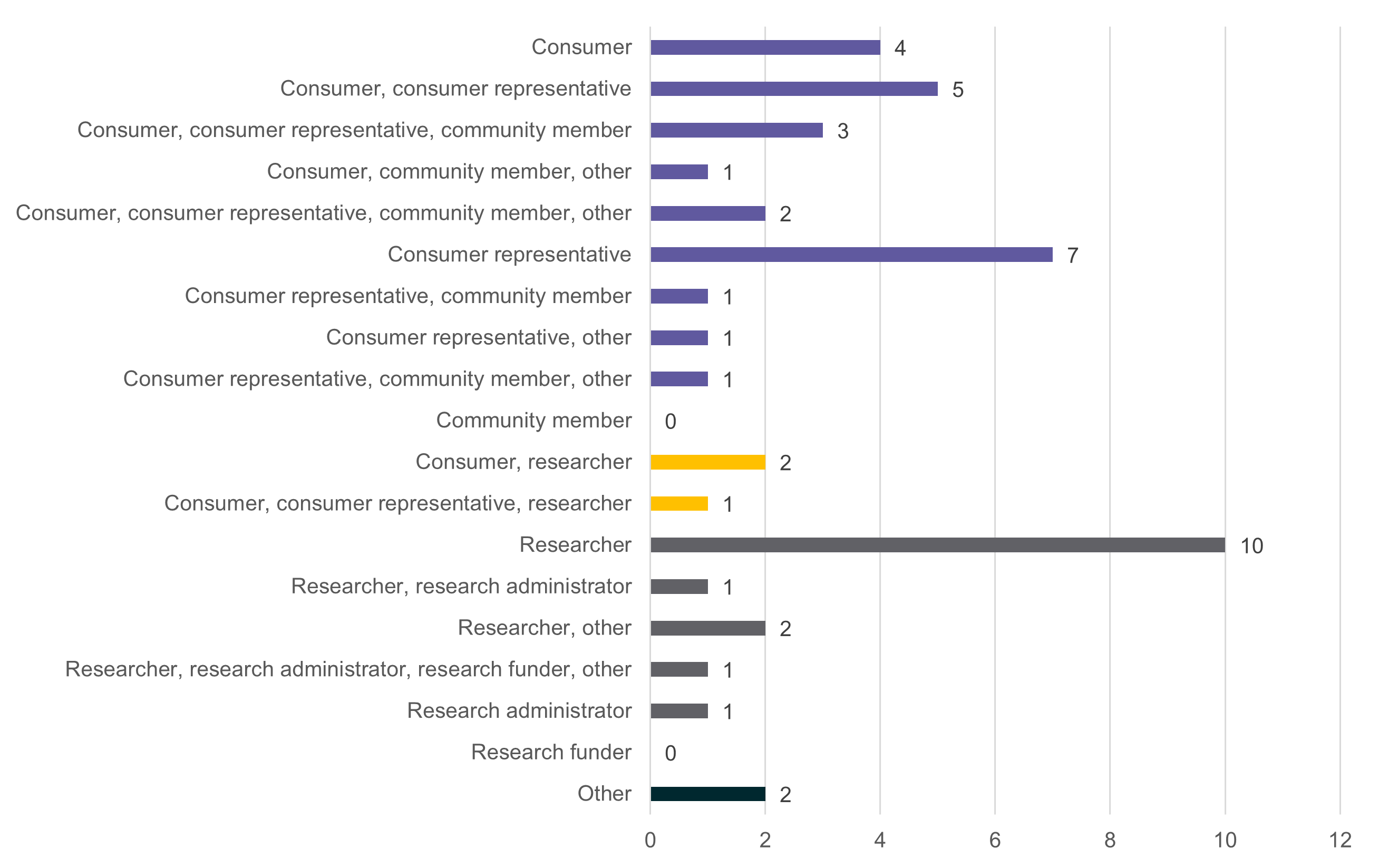
Stakeholder locations
The 45 individuals who responded to these questions were from all states and territories except for the Northern Territory. The greatest representation was from Queensland and Victoria (refer Figure 8), and from urban areas (refer Figure 9). At the AHRA-facilitated workshops, the greatest representation was from New South Wales (28% of attendees).
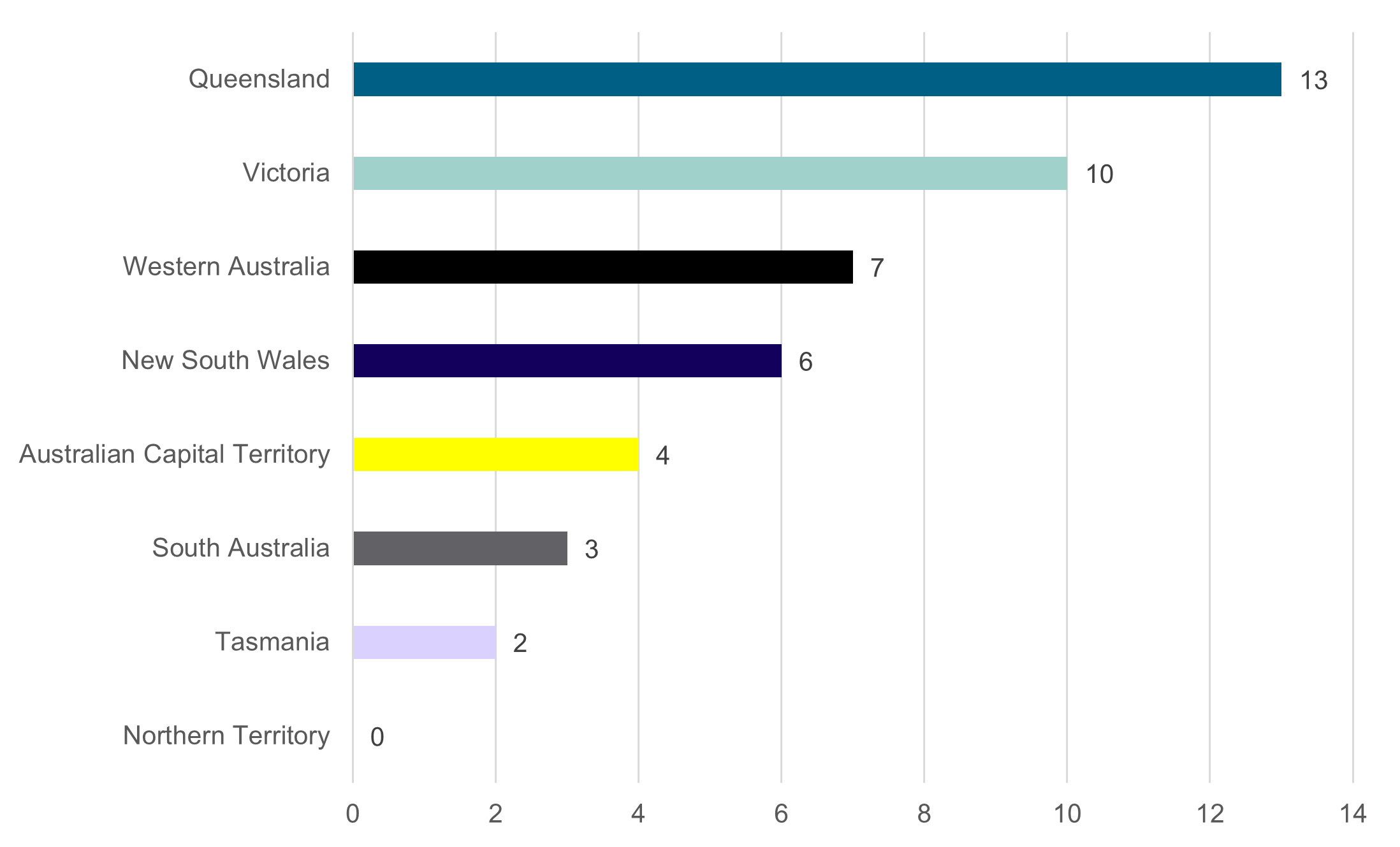
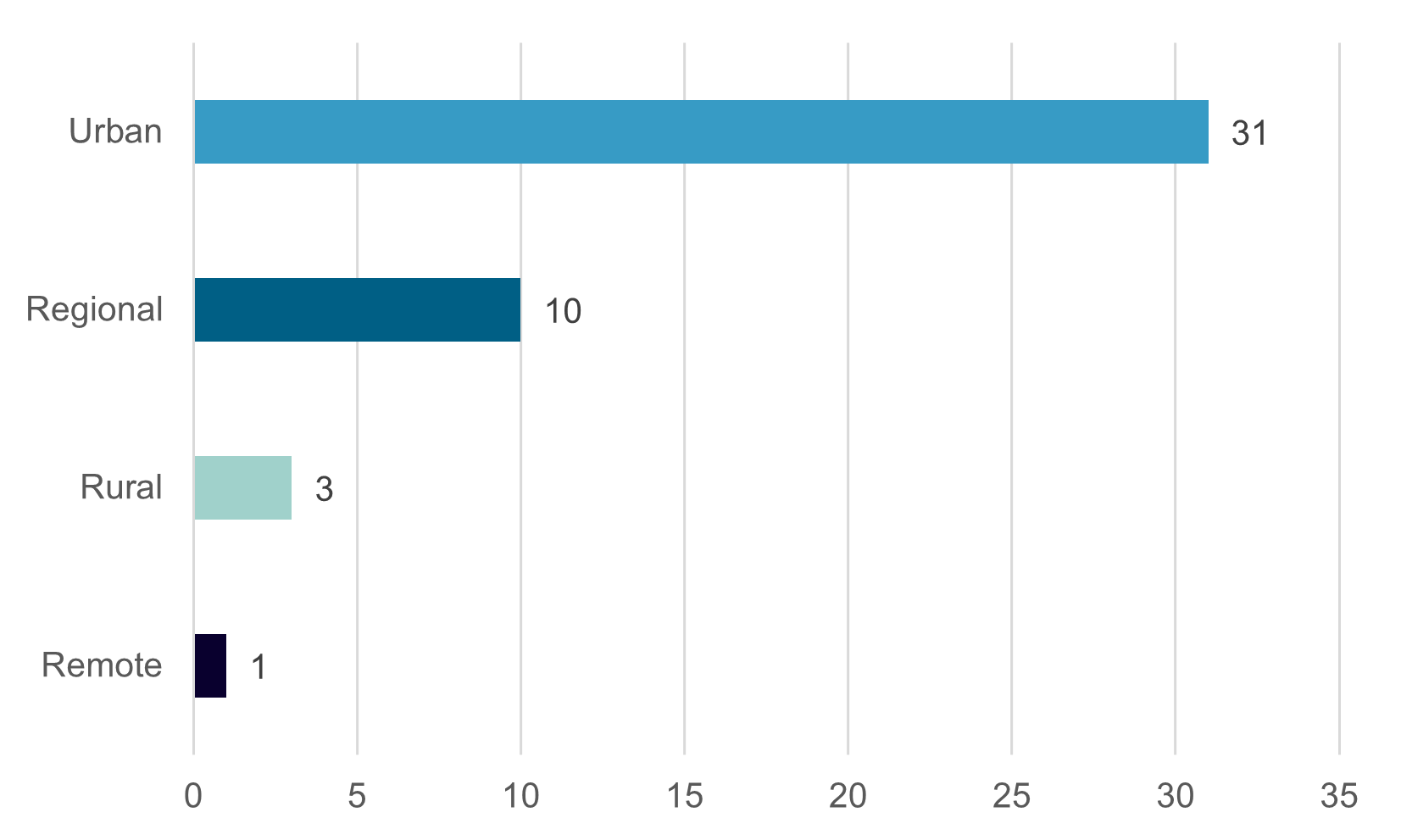
The majority of respondents to the remaining questions were born in Australia (n=31, 78%) and spoke only English at home (n=43, 96%). One respondent identified as Aboriginal.
Responses from organisations
Forty responses were received to the question 'is your organisation located in an urban, regional, rural or remote location?' Respondents could select multiple answers to reflect that organisations may have multiple locations (refer Figure 10). Of the organisations that provided a submission, 22 (55%) were in urban locations only, and one (2.5 was in a regional location only. Seventeen organisations (42.5%) had representation across some combination of urban, regional, rural and remote areas, with 10 organisations having locations in all areas.
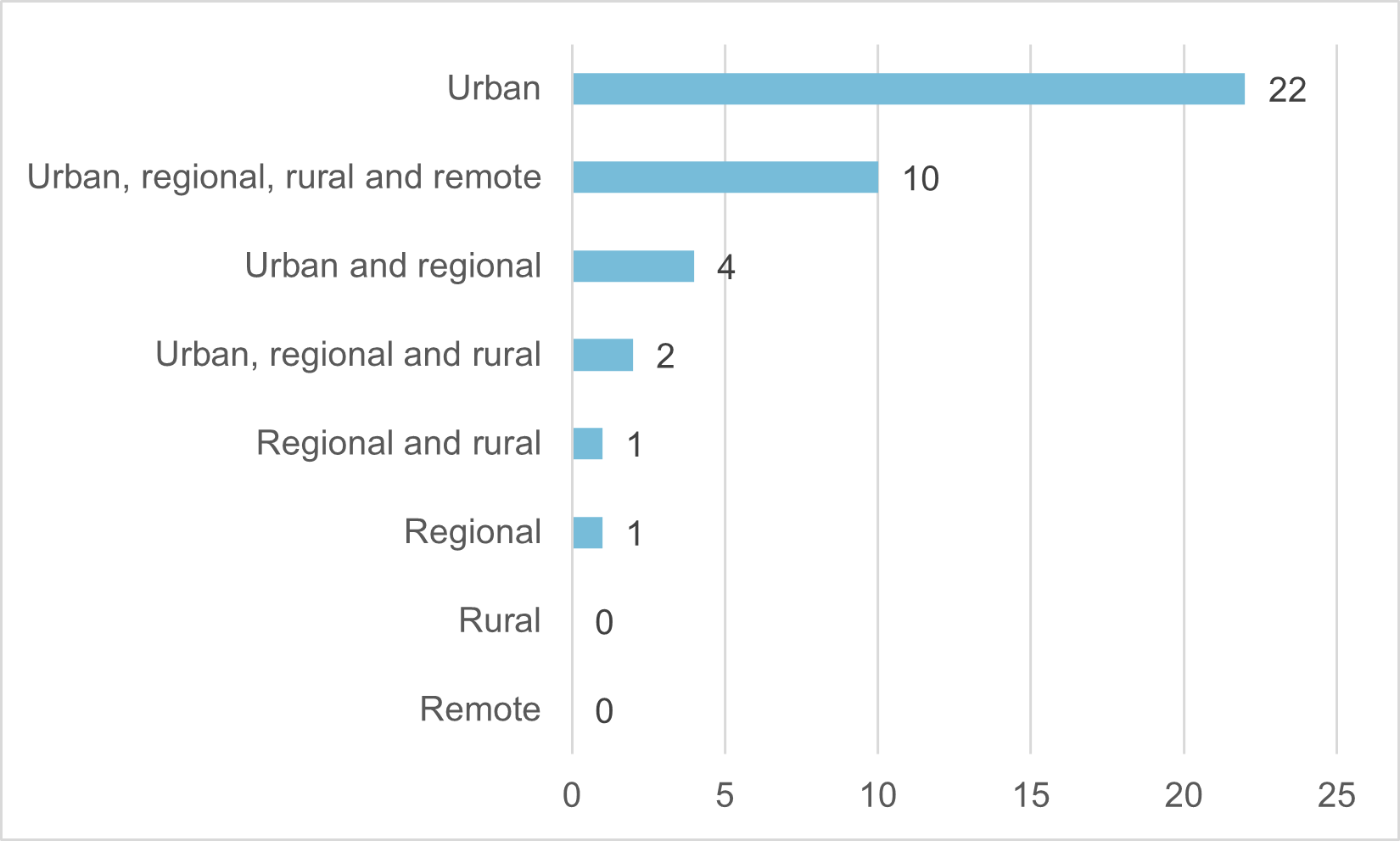
State and territory locations
Like the previous question, multiple states and territories could be selected in response to this question, acknowledging that some national bodies and organisations with multiple locations would be providing submissions. Of the 41 organisations that provided a submission, 26 (63%) were in a single state or territory only, and 15 (37%) had locations in multiple states or territories. Figure 11 shows the number of times each state and territory was selected in response to the question 'which state or territory is your organisation located in?'
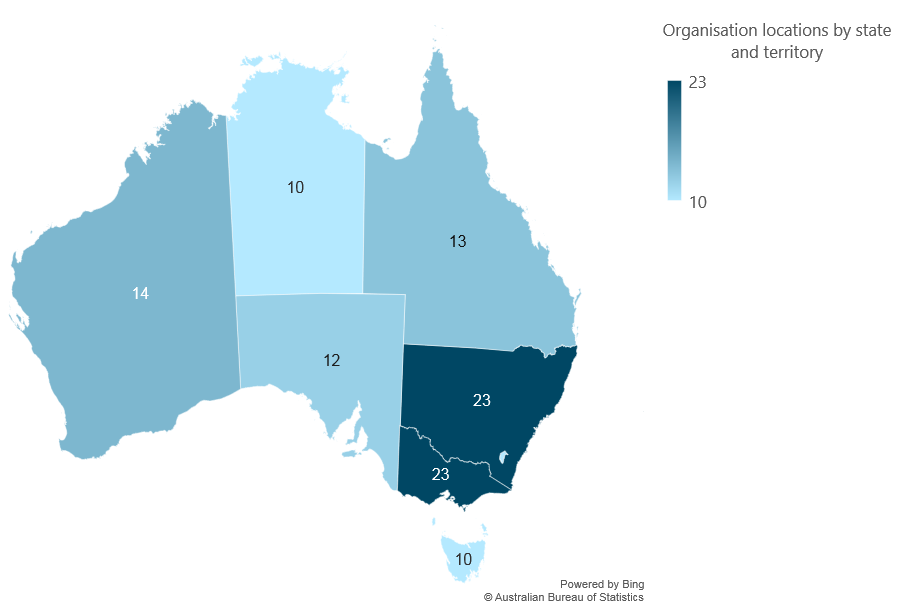
Appendix B - References
Stakeholders listed numerous existing publications, guidelines and standards that could be referred to when drafting a revised Statement. These are listed below, and grouped by the question they were mentioned in.
Question 1 – What parts of the current Statement have or have not worked well?
- Australian Clinical Trials Alliance (ACTA) - Toolkit for Researchers and Research Organisations: https://involvementtoolkit.clinicaltrialsalliance.org.au/toolkit/
- Diabetes Australia - Our Language Matters: https://www.diabetesaustralia.com.au/wp-content/uploads/Language-Matters-Diabetes-Australia-Position-Statement.pdf
- Health Consumers NSW and Sydney Health Partners - Language Guide for Consumer and Community Involvement in Health Research at Sydney Health Partners: https://cdn.sydneyhealthpartners.org.au/wp-content/uploads/2023/03/CCI-Language-Guide.pdf
- International Association for Public Participation – IAP2 Spectrum of Public Participation: https://www.iap2.org/page/pillars?
- National Breast Cancer Foundation - Consumers in grant review processes: https://nbcf.org.au/wp-content/uploads/2019/12/Consumers_and_Researchers_document_FINAL-for-web.pdf
- National Health and Medical Research Council - Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: Guidelines for researchers and stakeholders: https://www.nhmrc.gov.au/about-us/resources/ethical-conduct-research-aboriginal-and-torres-strait-islander-peoples-and-communities
- Sydney Health Partners - A Guiding Framework for Consumer and Community Involvement in Health Research at Sydney Health Partners: https://cdn.sydneyhealthpartners.org.au/wp-content/uploads/2023/03/CCI-Framework.pdf
- Telethon Kids Institute - Guidelines for the Standards for the Conduct of Aboriginal Health Research: https://www.telethonkids.org.au/our-research/Indigenous-health/aboriginal-research-standards/
- Victorian Comprehensive Cancer Centre (VCCC) Alliance - Model of Consumer Engagement: https://vcccalliance.org.au/consumer-engagement/model
Question 5 – The values that underpin the 2016 Statement are ‘shared understanding, respect and commitment.’ How might this be strengthened and improved in the revised Consumer Statement?
- Involve Australia – Guidelines for Community Involvement in Genomics Research: https://www.australiangenomics.org.au/wp-content/uploads/2021/06/Involve-Australia_Guidelines-for-Community-Involvement-in-Genomic-Research-1.pdf
- National Health and Medical Research Council - National Statement on Ethical Conduct in Human Research: https://www.nhmrc.gov.au/about-us/publications/national-statement-ethical-conduct-human-research-2023
- National Institute for Health and Care Research (NIHR) – Public involvement in research: values and principles framework: https://drive.google.com/file/d/0Bwij8ESXcoRbVjBVeW04OEdOWjA/view?resourcekey=0-iqB8X8C1SE_ItjodK04wOg
- National Institute for Health and Care Research (NIHR) – UK Standards for Public Involvement in Research: https://healthandcareresearchwales.org/sites/default/files/2023-11/UK_standards_for_public_involvement_11_2023.pdf
Question 7 – What do you regard as the most important principles that should be included in the revised Consumer Statement?
- Australian Institute of Aboriginal and Torres Strait Islander Studies - AIATSIS Code of Ethics for Aboriginal and Torres Strait Islander Research: https://aiatsis.gov.au/research/ethical-research
- Cancer Australia - National Framework for Consumer Involvement in Cancer Control: https://www.canceraustralia.gov.au/sites/default/files/migrated-files/publications/national_consumer_framework_web_504af020f2184.pdf
- Department of Health and Aged Care – National Consumer Engagement Strategy for Health and Wellbeing: https://www.health.gov.au/news/national-consumer-engagement-strategy-for-health-and-wellbeing
- Department of Health and Aged Care – Principles for Consumer Involvement in Research Funded by the Medical Research Future Fund: https://www.health.gov.au/resources/publications/principles-for-consumer-involvement-in-research-funded-by-the-medical-research-future-fund?language=en
- Health Care Consumers - Consumer and Community Participation Framework: https://www.hcca.org.au/publication/consumer-and-community-participation-framework/
- Health Consumers Queensland - Consumer and Community Engagement Framework for Health Organisations and Consumers: https://www.hcq.org.au/guides/
- Matilda Centre PREMISE Youth Advisory Board – Principles for Youth Engagement in Mental Health and Substance Use Research: https://www.nhmrc.gov.au/about-us/resources/ethical-conduct-research-aboriginal-and-torres-strait-islander-peoples-and-communities
- NHS Health Research Authority – Public Involvement: https://www.hra.nhs.uk/planning-and-improving-research/best-practice/public-involvement/
- Stakeholder Engagement in Research: The Research-Modified IAP2 Spectrum: https://i2insights.org/2020/01/07/research-modified-iap2-spectrum/ (note: this has been superseded by the Stakeholder Engagement Primer: 4. Options for Engagement: https://i2insights.org/2021/11/04/options-for-engagement/)
- UNSW Disability Innovation Institute - Doing Research Inclusively: Guidelines for Co-Producing Research with People with Disability: https://www.disabilityinnovation.unsw.edu.au/inclusive-research/guidelines
Questions 8-11 – What roles and responsibilities for consumers and community members, researchers, research institutions and research funders should be included in the revised Consumer Statement?
- Arnstein L et al. - Patient involvement in preparing health research peer-reviewed publications or results summaries: a systematic review and evidence-based recommendations: https://researchinvolvement.biomedcentral.com/articles/10.1186/s40900-020-00190-w
- Australian Clinical Trials Alliance – Consumer Involvement and Engagement Toolkit: https://involvementtoolkit.clinicaltrialsalliance.org.au/
- Australian Commission on Safety and Quality in Healthcare - National Clinical Trials Governance Framework and User Guide: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/national-clinical-trials-governance-framework-and-user-guide
- Involve Australia - Recommendations for health and medical research funders to support community involvement in research: https://www.australiangenomics.org.au/wp-content/uploads/2021/06/Involve-Australia_Recommendations-for-funders_May-2024.pdf
- Involve Australia - Recommendations for health and medical research institutes to support community involvement in research: https://www.australiangenomics.org.au/wp-content/uploads/2021/06/Involve-Australia_Recommendations-for-institutes_May-2024.pdf
- Western Australian Health Translation Network - Involving Consumers in Health and Medical Research: A practical handbook for organisations, researchers, consumers and funders: https://wahtn.org/platforms/consumer-and-community-involvement/cci-handbook/
- Woolley KL et al. - Patient authorship of medical research publications: An evolution, revolution, and solution? https://onlinelibrary.wiley.com/doi/full/10.1002/leap.1607
Footnotes
1 Statement on consumer and community involvement in health and medical research | NHMRC
2 The Position Paper and Environmental Scan are available at: Consultation activities
3 The AHRA report is available at: Consultation activities
4 Some responses have been amended for readability.
5 Wordstat by Provalis Research
6 Principles for consumer involvement in research funded by the Medical Research Future Fund | Australian Government Department of Health and Aged Care
7 UK Standards for Public Involvement | NIHR
8 Principles of Community Engagement (Second Edition) (cdc.gov)
9 Australian Code for the Responsible Conduct of Research 2018 | NHMRC
10 National Framework for Consumer Involvement in Cancer Control | Cancer Australia
11 NOTE: This Strategy has been superseded by: Patient and Public Involvement, Engagement and Participation (PPIE) Strategy 2022-2027 - Cambridge Biomedical Research Centre (nihr.ac.uk)
12 Lived experience involvement in research funding: taking a more systematic approach | Nature Mental Health
13 Public Involvement - Health Research Authority (hra.nhs.uk)